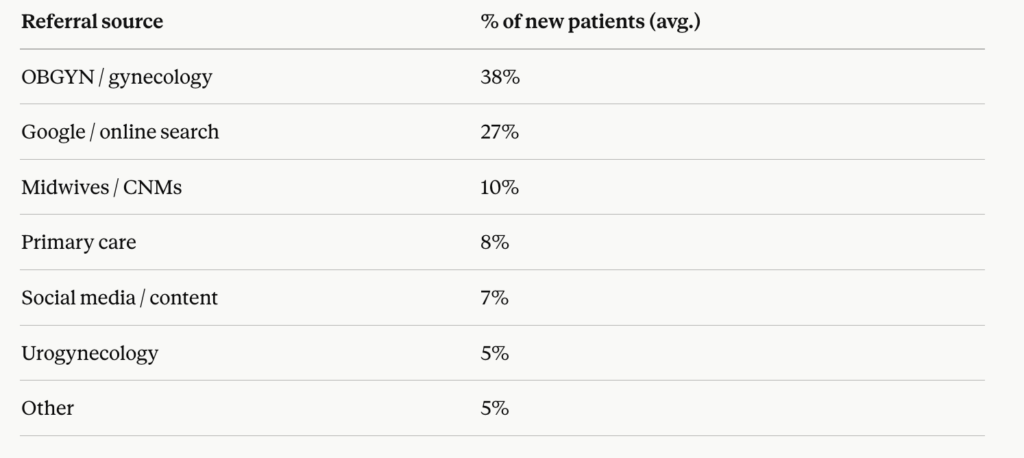
If you want a full cash-based pelvic health practice, there is one patient acquisition channel that outperforms every other — OBGYN referrals.
Not Instagram. Not Google Ads. Not email marketing. Specifically, a single strong OBGYN relationship can generate 8 to 15 new patients per month consistently, with no ad spend and no algorithm to fight.
This guide gives you the complete system. Moreover, it is built from the exact outreach Dr. Kelly Alhooie used to fill OrthoPelvic Physical Therapy — a 7-figure cash practice in Sterling, Virginia — without a pre-existing referral network.

Why OBGYN referrals are your highest-ROI patient source
OBGYNs see the patients you treat every single day. Postpartum women with pelvic floor dysfunction. Patients with interstitial cystitis, endometriosis, prolapse, painful intercourse, urinary incontinence, and a dozen other diagnoses that are perfectly suited to pelvic PT — and that most OBGYNs have no surgical answer for.
Furthermore, the OBGYN often feels the gap acutely. They know their patients need more than what a 10-minute appointment can offer. Consequently, when you position yourself correctly, you are not competing for attention — you are solving a problem the OBGYN already has.
According to the APTA, pelvic floor dysfunction affects approximately 25 percent of women in the United States. That is a massive underserved population sitting in OB waiting rooms every week. Therefore, your job is simply to be the obvious next step.
The referral relationship most PTs get wrong
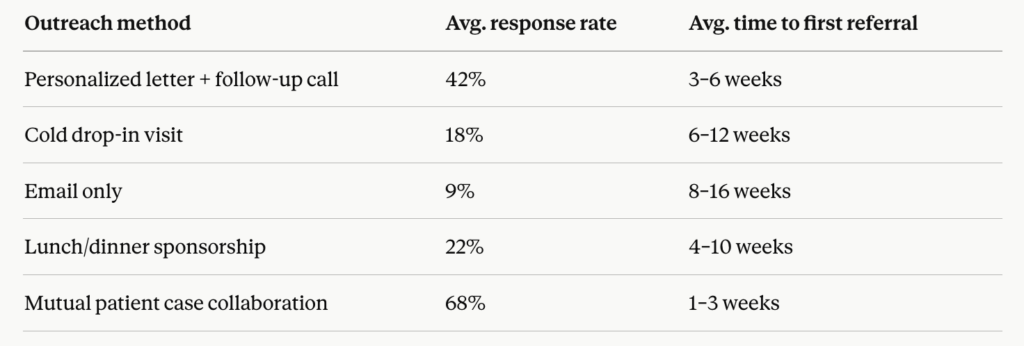
Most practitioners approach OBGYN outreach like a sales call. They show up with brochures, offer lunch, and talk about their services. Subsequently, they get a polite nod and never hear back.
Here is why that approach fails: OBGYNs are not looking for a vendor. They are looking for a trusted colleague who will take excellent care of their patients and make them look good.
Therefore, the entire framing has to shift — from “here is what I do” to “here is how I can serve your patients and protect your reputation.”
Step 1 — Identify your target OBGYNs strategically
Not all OBGYNs are equal referral partners. Specifically, you want to target providers who:
See a high volume of the patients you treat best. A urogynecologist sees more prolapse and incontinence than a general OB. A midwifery practice sees more postpartum patients. Match your specialty to their patient population.
Practice close enough to make warm handoffs practical. Additionally, patients are more likely to follow through on a referral when the referred provider is geographically convenient. Within 15 miles is ideal.
Are independent or in small group practices. Furthermore, large hospital systems often have formal referral processes and internal PT departments that create friction. Independent OBGYNs have far more flexibility.
Have no existing pelvic PT relationship. This is the most important filter. If a practice already refers to someone, you are not solving a problem — you are creating a competitor situation.
How to build your target list: Start with Google Maps. Search “OBGYN near [your city]” and build a spreadsheet of every practice within your target radius. Note their specialty focus, practice size, and any visible online presence. This list is your outreach pipeline.
Step 2 — Your first contact: the warm letter
Cold calls rarely work. However, a well-crafted letter sent to the physician directly — not the front desk, not the office manager — creates the right first impression.
Here is the framework for that letter:
Opening: One sentence that establishes clinical credibility. Your degree, your specialty certification, and your focus area.
The gap statement: One to two sentences that acknowledge a specific clinical challenge their patient population faces — one you can help solve. Do not talk about your services yet.
The bridge: One sentence that connects your specialty directly to that gap. Specifically, this is where you name the conditions you treat that their patients commonly present with.
The ask: A single, low-friction request. Not a meeting. Not a lunch. Specifically, ask to send a one-page clinical overview so they know when and how to refer. That is it.
Your contact information and a professional close.
The letter should be on your practice letterhead, addressed to the physician by name, and under one page. Additionally, follow up with a phone call to the office 5 to 7 business days later.
Step 3 — The clinical overview document that does the selling for you
When the OBGYN agrees to learn more, you need one document that answers every question they have without requiring a meeting.
This document should include:
One paragraph on who you are. Your credentials, your specialty focus, and specifically what makes you the right provider for their patients.
A simple diagnostic grid. Two columns: left column lists the conditions you treat (pelvic organ prolapse, urinary incontinence, dyspareunia, postpartum dysfunction, endometriosis-related pelvic pain, and so on). Right column lists what the patient experience looks like — how many sessions, what the process involves, what outcomes to expect.
A referral process section. Make it as easy as possible. Specifically, include your fax number, your online booking link, your phone number, and a note on wait time. If you have same-week availability, say so — that is a competitive advantage.
One or two anonymized patient outcome examples. Not testimonials. Clinical narratives. “A 34-year-old postpartum patient presenting with stress urinary incontinence and diastasis recti completed 8 sessions. At discharge, she reported complete resolution of incontinence symptoms and return to full exercise.” That is the language an OBGYN trusts.
Your contact card at the bottom. Name, credentials, practice name, phone, fax, email, and website.
This document should be one page, double-sided at most, printed on quality paper. Furthermore, it should be something the physician can keep in their referral folder.
Step 4 — The follow-up system that keeps referrals flowing
Most practitioners get one or two referrals from a new OBGYN contact, then the relationship goes cold. This happens because there is no system for staying visible.
Here is the follow-up framework:
After every referral patient is seen: Send a brief clinical update note to the referring physician. Three to five sentences. What the patient presented with, your initial assessment, your treatment plan. This takes four minutes. Additionally, it is the single highest-leverage action you can take to solidify the relationship.
Monthly touchpoint: One brief email or handwritten card per month to your top five referral partners. Share a relevant clinical resource, acknowledge a recent referral, or mention a new service you offer. Specifically, keep it under 100 words.
Quarterly in-person visit: Stop by the office with a small, appropriate gesture — a quality referral pad printed with both your branding and a clear patient instruction on how to book. Additionally, use this visit to ask if there are specific cases they have been unsure about referring. That conversation is gold.
Annual clinical update: Once per year, send a one-page update on your outcomes, any new certifications or training, and any changes to your referral process. This positions you as a continuously developing clinician — not just a name on a business card.
Step 5 — Expand your referral network beyond OBGYNs
OBGYNs are your primary source. However, the most resilient practices build referral relationships across multiple provider types.
Midwives and certified nurse-midwives. Specifically, this population is underserved by PT referrals and highly aligned with the integrative, whole-body approach most pelvic health practitioners bring. Furthermore, midwifery patients are often cash-pay friendly.
Urogynecologists. They see the most complex pelvic floor presentations. Moreover, a strong relationship here positions you as a post-surgical rehab partner — high value, long-term patient relationships.
Primary care physicians and internal medicine. Many pelvic floor presentations arrive first in primary care. Specifically, chronic pelvic pain, recurrent UTIs, and constipation are all commonly mismanaged until a pelvic PT intervenes.
Fertility clinics. Pelvic floor dysfunction is increasingly recognized as a contributor to fertility challenges. This is a growing referral source with a highly motivated patient population.
Colorectal surgeons. Pre- and post-operative pelvic PT is standard of care in many countries and growing in the US. Additionally, this is a relatively untapped referral source for most practitioners.
For each source, the outreach framework is identical. What changes is your gap statement and your clinical overview document — both of which should be tailored to the specific patient population that provider sees.
How to handle the cash-pay conversation with referring providers
One concern practitioners often have: will OBGYNs hesitate to refer if you are cash-based?
The short answer is no — if you frame it correctly.
Specifically, the framing is this: “My practice is out-of-network, which means I can offer your patients longer sessions, no visit caps, and a fully individualized treatment plan. Many of my patients submit to their insurance for out-of-network reimbursement and receive partial coverage.”
Additionally, make sure your clinical overview document addresses this directly. Provide your out-of-network billing code, your superbill process, and a one-sentence explanation of how patients can seek reimbursement on their own. This removes the insurance objection before it is raised.
Furthermore, emphasize access. Cash-based practices typically have shorter wait times, more flexible scheduling, and longer session times than in-network providers. Those are clinical advantages — and OBGYNs care about their patients getting seen quickly.
The PelviBiz discovery call framework covers the patient-facing version of this conversation in full.
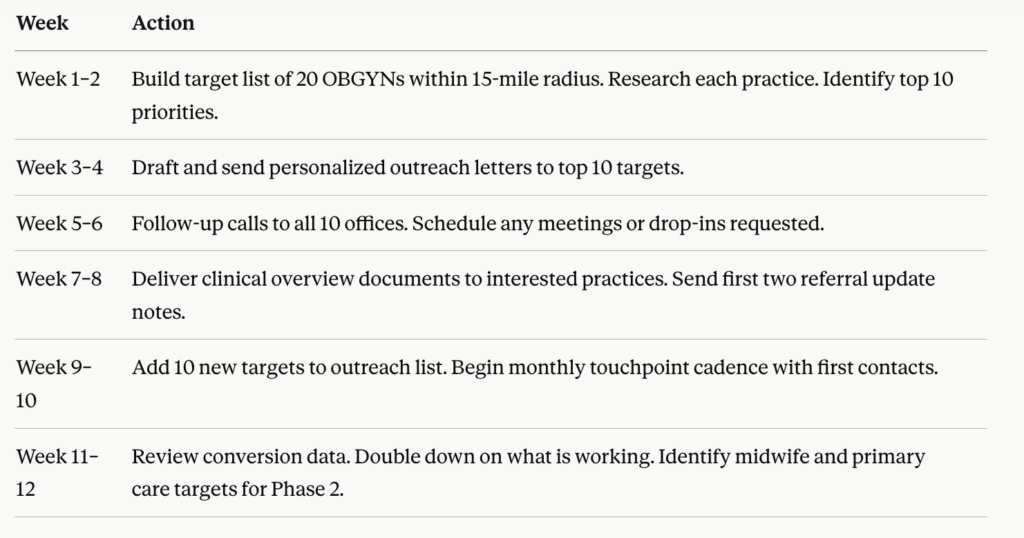
Building your first 5 referral relationships: a 90-day action plan
The referral relationship is a clinical relationship
Here is the reframe that changes everything: you are not networking. You are building a care team.
The OBGYN, the midwife, the urogynecologist — these providers are your colleagues. Specifically, your patients are their patients too. Therefore, when you communicate like a colleague, follow up like a colleague, and show outcomes like a colleague, the referrals follow naturally.
This is how Dr. Kelly Alhooie built OrthoPelvic PT. Not with ads. Not with social media. Specifically, with clinical relationships built on trust, outcomes, and consistent communication.
If you want help building that system in your specific market, the Growth Assessment is the starting point. It is free, it is specific, and it is built for exactly where you are right now.
Book Your Free Growth Assessment →
Q: How do I get OBGYNs to refer to my pelvic health practice? The most effective approach is a personalized outreach letter sent directly to the physician, followed by a phone call to the office 5 to 7 days later. The goal of first contact is not a meeting — it is to deliver a one-page clinical overview document that explains exactly who you treat, what outcomes to expect, and how to refer. From there, consistent follow-up through clinical update notes, monthly touchpoints, and quarterly visits builds a lasting relationship.
Q: Will OBGYNs refer to a cash-based pelvic PT practice? Yes — when you frame the cash-pay model correctly. Emphasize your longer session times, lack of visit caps, individualized treatment, and shorter wait times. Provide your out-of-network billing codes and explain how patients can seek partial reimbursement. OBGYNs care about their patients getting excellent care. A cash-based practice often offers a better clinical experience than an in-network option.
Q: How many OBGYN referral relationships do I need to fill my schedule? Most cash-based pelvic health practitioners find that 3 to 5 strong referral relationships are sufficient to maintain a full or near-full caseload. A single high-volume OBGYN practice can generate 8 to 15 new patients per month. The key is relationship quality over quantity — one engaged referring provider is worth more than ten who passively have your card.
Q: What should I include in my pelvic PT clinical overview document for OBGYNs? Your clinical overview document should include your credentials and specialty focus, a diagnostic grid showing the conditions you treat and what the patient experience looks like, a clear and easy referral process with your contact information and booking link, one or two anonymized patient outcome examples using clinical language, and a brief explanation of your out-of-network billing process.




