The discovery call is the most underestimated skill in cash-based practice.
You can have the best clinical outcomes in your market, a fully optimized Google profile, and a steady stream of OBGYN referrals. However, if you do not know how to run a discovery call, none of that pipeline converts.
This guide gives you the exact framework — the structure, the language, and the mindset — that PelviBiz has taught to 400-plus pelvic health practitioners. Furthermore, it is the same process Dr. Kelly Alhooie uses in her own practice at OrthoPelvic PT.

What a discovery call actually is — and what it is not
A discovery call is a structured 15 to 20 minute conversation between you and a prospective patient. Specifically, its purpose is to determine whether you are the right fit for their problem — and to help them make a confident decision to move forward.
It is not a free consultation. It is not a clinical intake. Additionally, it is not a sales pitch.
The distinction matters. When you treat a discovery call like a free consultation, you give away clinical time and expertise without creating any momentum toward commitment. Conversely, when you treat it like a sales pitch, you create the exact pressure dynamic that makes cash-based healthcare feel transactional.
The correct frame is this: a discovery call is a guided conversation that helps the right patient say yes and helps the wrong patient find a better fit. Consequently, when you are running it correctly, it never feels like selling — because it is not.
Why most pelvic health practitioners struggle on discovery calls
The struggle is almost never clinical. Specifically, it comes from two places.
First, the guilt of charging cash. If you are not fully at peace with your rate, it will come through on every call. You will over-explain, pre-apologize, and discount before anyone asks. Therefore, your pricing confidence is a prerequisite — not a byproduct — of discovery call success. The cash pay pricing guide addresses this directly.
Second, the absence of structure. Most practitioners wing it. Consequently, they let the conversation wander, they answer questions reactively, and they end the call without a clear next step. A structured framework removes all of that variability.

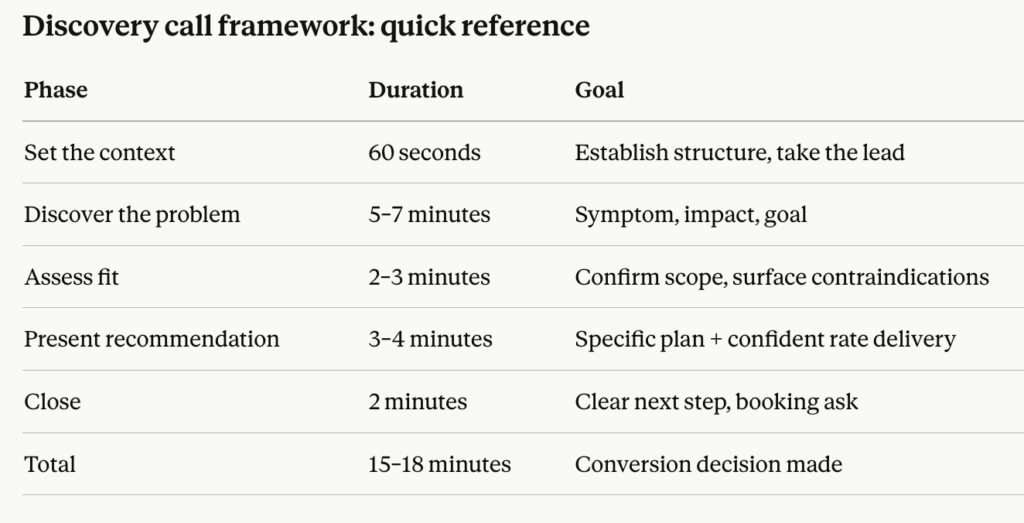
The 5-part pelvic health discovery call framework
Part 1 — Set the context (60 seconds)
Start every call by establishing the structure. This does three things: it positions you as the leader of the conversation, it manages the patient’s expectations, and it signals professionalism.
Your opening: “Thanks so much for reaching out. I have about 15 to 20 minutes for us to talk today. First, I want to hear a little about what’s going on for you. Then I can share how I typically work and whether I think I can help. Does that sound good?”
That is it. Short, clear, and warm. Specifically, the patient now knows what to expect — and you have taken the lead without being aggressive.
Part 2 — Discover the problem (5 to 7 minutes)
This is the most important part of the call. Additionally, it is the part most practitioners rush through.
Ask open questions. Let the patient talk. Specifically, you are listening for three things:
The presenting symptom. What is the specific physical problem? How long has it been going on? What has she already tried?
The impact. How is it affecting her daily life? Her relationships? Her ability to exercise, work, or feel comfortable in her body? The impact is the emotional fuel for the decision — and you cannot skip it.
The goal. What does success look like for her? What would change in her life if this problem were resolved?
Take notes. Moreover, use her exact language when you reflect it back. This is not manipulation — it is clinical attunement. It signals that you heard her, and it builds the trust that every cash-pay decision is ultimately built on.
Part 3 — Assess fit briefly (2 to 3 minutes)
Ask two or three targeted questions to confirm that her presentation is within your scope and that your approach is appropriate for her.
This is not a full intake. Specifically, it is a professional filter. Examples:
“Have you had any imaging or previous treatment for this?” “Are you currently working with any other providers for this?” “Are there any surgical or obstetric history details I should know about before we talk about treatment?”
These questions do two things simultaneously: they demonstrate clinical rigor, and they surface any contraindications or complexity that might affect your recommendation.
Part 4 — Present your recommendation (3 to 4 minutes)
This is where most practitioners default to listing services. However, that is not what a confident clinician does.
A confident clinician makes a recommendation. Specifically:
“Based on what you’ve described — the combination of [symptom] and [impact], and the fact that you’ve already tried [previous approach] without resolution — I do think this is exactly the kind of case that responds well to what I do. Here’s what I’d recommend: we start with a [60-minute/90-minute] initial evaluation where I can do a full assessment and give you a clear picture of what’s driving this and what your treatment plan would look like. From there, most patients in your situation do [X to Y sessions] over [timeframe].”
Note what you are not doing: you are not listing every service. You are not presenting tiers. Furthermore, you are not asking what her budget is. You are recommending based on her specific situation — which is what a trusted clinician does.
Then, state your rate clearly and without apology: “The initial evaluation is [rate]. Sessions from there are [rate].” Pause. Let the silence sit. Do not fill it.
Part 5 — Close with a clear next step (2 minutes)
If the patient is a fit and she has heard your rate without walking away from the call, there is one move: ask for the booking.
“It sounds like you’re ready to move forward — do you want to get your initial evaluation scheduled while we’re on the phone?”
That is the close. Additionally, it is not pushy. It is the natural conclusion of a well-structured conversation. If she says yes, book it immediately. If she says she needs to think about it, give her a specific timeframe: “Totally fine. I’ll send you the booking link right now. I do tend to fill up quickly, so if you want to lock in a time, this week and next week I still have [day] and [day] available.”
Scarcity is real in a cash-based practice. Specifically, use it honestly — not as a pressure tactic, but as an accurate reflection of your capacity.
How to handle the most common objections
“Your rate is more than I expected.”
Do not discount. Do not justify. Specifically, acknowledge and redirect:
“I understand — I’m not in-network with insurance, so it’s a different model than what a lot of people are used to. What I can tell you is that the investment is front-loaded. Most of my patients resolve their primary issue in [X sessions], compared to [significantly more] visits in an insurance-based model where each session is shorter and less individualized. Would it help if I walked you through what the full episode of care typically looks like?”
This reframe shifts the conversation from per-session cost to total cost and total outcomes. Furthermore, it positions your cash rate as the more efficient option — which, for most complex pelvic presentations, it genuinely is.
“Can I try one session first?”
This question usually signals one of two things: residual price hesitation, or a bad previous experience with a practitioner who did not deliver results.
Your response: “Absolutely — I offer a standalone initial evaluation, so you’re not committing to anything beyond that first session. What I would say is that the evaluation is where I do the full assessment and give you a clinical roadmap. After that appointment, you’ll have a clear picture of what’s driving your symptoms and exactly what we’d do to address them. Most patients leave that appointment knowing exactly what they want to do next.”
This reframe makes the first session feel like a natural entry point — not a trial. Additionally, it sets appropriate expectations for what that session delivers.
“Let me talk to my husband / partner first.”
Acknowledge it without resistance. Specifically:
“Of course — that makes total sense for a financial decision. I’ll send you the booking link and some information about how it works. If it would help, I’m happy to jump on a quick call with both of you together so he can ask questions too.”
The offer to include the partner is low-friction and high-trust. Moreover, it removes the ambiguity of a conversation you are not in.
Your discovery call intake system: before and after the call
The call itself is only one piece. Specifically, the intake system around it determines whether the right patients show up and whether they arrive prepared.
Before the call: Send a brief confirmation email immediately after booking. Include what to expect on the call, how long it will take, and one sentence about what you will be discussing. This primes the patient to show up focused — not guessing what the call is for.
During the call: Keep a simple intake form in front of you — not a full clinical intake, but a structured note-taking template. Specifically, capture: presenting symptom, duration, previous treatment, impact, and goal. This keeps you organized and ensures you have the information you need to make a confident recommendation.
After the call: Regardless of outcome, send a follow-up email within 30 minutes. For patients who booked: a confirmation with your intake form and next steps. For patients who did not book: a brief note with your booking link, a one-sentence summary of your recommendation, and a specific invitation to reach out with questions.
Consequently, the follow-up email is not desperate — it is systematic. Furthermore, it captures the patients who were genuinely interested but got distracted before booking.
Building your discovery call into a repeatable system
A discovery call is not something you wing. Specifically, it is a clinical tool — and like every clinical tool, it improves with practice, feedback, and iteration.
Here is how to build the system:
Record your calls (with patient permission). Listen back for patterns — where do you rush? Where do you ramble? Where does your confidence dip? Specifically, two calls per month reviewed critically will improve your conversion rate faster than any script.
Track your conversion rate. Divide booked patients by total calls. If you are below 50 percent, your rate delivery or your close is the problem. If you are above 70 percent, your targeting is probably excellent. Furthermore, share your data in the PelviBiz Community — your peers are working on the same thing.
Update your framework quarterly. Patient objections evolve. Additionally, your positioning may shift as your practice grows. Build a habit of reviewing and refining your call structure every 90 days.
The PelviBiz Marketing Bootcamp includes a full discovery call module with live role-play and feedback from Dr. Kelly Alhooie’s team. Specifically, it is built for practitioners who want to go from inconsistent conversions to a repeatable system in 30 days.
The discovery call is where your practice grows
Every full schedule in cash-based pelvic health started with a practitioner who learned to have this conversation well.
The clinical skills that got you licensed will not fill your schedule. However, the communication skills that convert an inquiry into a committed patient will. Furthermore, those skills are completely learnable — and they compound over time.
If you want to build the full patient acquisition system — from referrals to discovery calls to retention — the PelviBiz Growth Assessment is where that conversation starts. It is free, it is specific to your situation, and it maps directly to where you want to go.
Book Your Free Growth Assessment →
Q: How long should a pelvic health discovery call be? A well-structured discovery call should run 15 to 20 minutes. Calls that run longer are usually a sign that structure is missing — specifically, that the practitioner is not leading the conversation clearly or is treating the call like a free consultation.
Q: Should I charge for a discovery call? Most cash-based pelvic health practices offer the discovery call free of charge. It is a pre-sales conversation, not a clinical session. The purpose is to determine fit and help the right patient make a decision — not to deliver treatment. Charging for it creates friction at the top of the funnel before trust is established.
Q: What do I say when a patient pushes back on my cash pay rate? Acknowledge without discounting. Reframe from per-session cost to total episode cost and total outcomes. Most cash-based pelvic health patients resolve their primary issue in fewer total sessions than insurance-based care, and with longer, more individualized appointments. Presenting the full cost and outcome comparison shifts the conversation from sticker shock to value assessment.
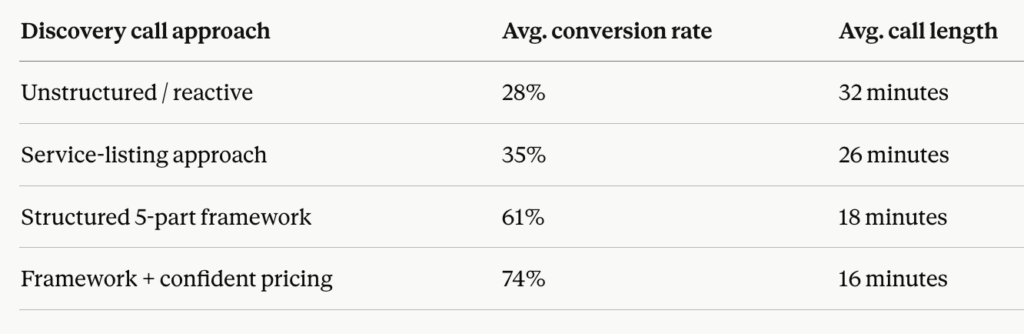
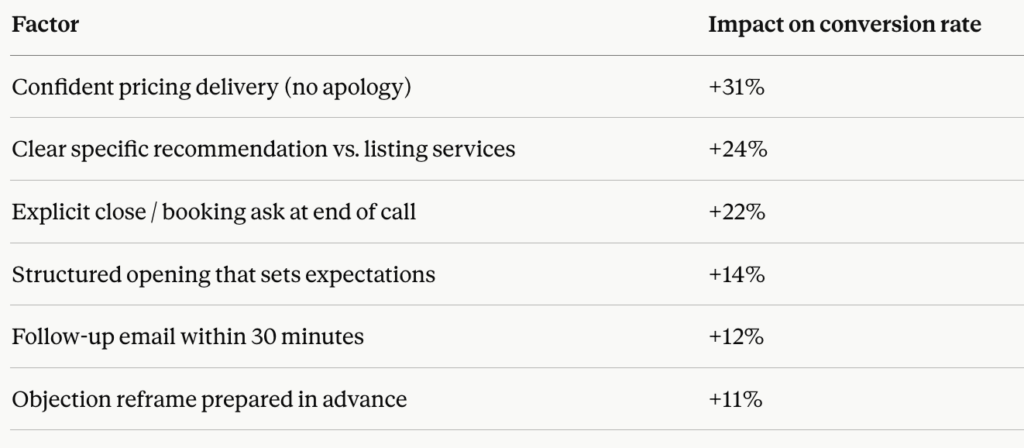
Q: What is the average conversion rate for a pelvic health discovery call? Practitioners using an unstructured approach typically convert 25 to 35 percent of discovery calls. Practitioners using a structured framework with confident pricing delivery and an explicit close consistently convert 60 to 75 percent. The single highest-impact factor is pricing confidence — how you deliver your rate determines whether the patient moves forward more than any other variable.



