If you are thinking about moving from insurance to cash pay, you are not alone — and you are not crazy. You are finally asking the right question.
The insurance model was never built for practitioners like you. It was built for volume. Therefore, every system inside it — the billing codes, the productivity metrics, the documentation requirements — pushes you toward seeing more patients in less time for less money. That is the opposite of what a sustainable, profitable pelvic health practice looks like.
This guide gives you the exact framework for making the switch. Furthermore, it is the same framework Dr. Kelly Alhooie used to build OrthoPelvic Physical Therapy into a 7-figure cash-based practice in Sterling, Virginia — from scratch, with no referral base, no name recognition, and no roadmap.

Why practitioners are leaving insurance in record numbers
The data is not subtle. According to the American Medical Association, physician practice ownership has declined significantly over the past decade — and insurance reimbursement rates are a primary driver. For physical therapists, the math is even more unforgiving.
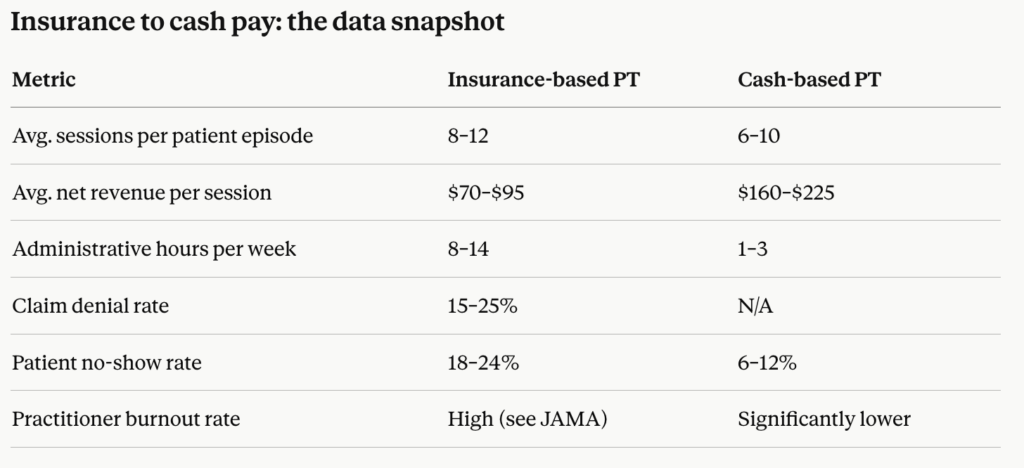
However, the practitioners who have made the switch consistently report the same outcome: more revenue per session, fewer administrative hours, and a better clinical experience for every patient they see. Specifically, cash-based practices eliminate prior authorizations, claim denials, and the endless cycle of documentation that has nothing to do with patient outcomes.
The Bureau of Labor Statistics projects consistent demand for physical therapy services through 2032. That demand exists whether you bill insurance or not. The question is simply who captures the value — you or the insurer.
The biggest myth about going cash pay
Most practitioners believe that going cash pay means losing patients. Consequently, they stay stuck in a system that is quietly draining them.
Here is the truth: you will lose some patients. Additionally, the ones you keep will be better patients — more committed, more compliant, and more likely to refer. Moreover, your revenue per session will increase substantially, which means you need fewer sessions to hit the same monthly income.
Dr. Kelly Alhooie talks about this directly in the PelviBiz Podcast. The transition is not about charging more for the same thing. It is about delivering a premium clinical experience that insurance never allowed you to deliver in the first place.

The insurance to cash pay transition: your phase-by-phase framework
Phase 1 — Run the real numbers first
Before you hand in your notice or drop your first panel, you need a clear financial picture. Specifically, here is what to calculate:
Your current effective hourly rate. Take your total monthly income and divide it by every hour you spend working — including documentation, billing follow-up, and meetings. Most insurance-based PTs are shocked to find their effective rate is well below their billed rate.
Your cash pay break-even point. If you currently see 25 patients per week at a net insurance rate of $80 per session, that is $2,000 per week. Furthermore, at a cash rate of $175 to $225 per session, you need only 9 to 12 patients per week to match that income. Consequently, you do not need a full caseload to survive the transition.
Your runway. How many months of expenses can you cover while you build? Three months is the minimum. Six is comfortable. Therefore, your transition timeline should be built around your runway, not your emotions.

Phase 2 — Set your cash pay pricing with confidence
Pricing is where most practitioners freeze. However, there is a system for this.
First, anchor your rate to outcomes — not to insurance reimbursement. Insurance rates were set by actuaries to manage risk across large populations. They have nothing to do with the value you deliver to an individual patient who is finally able to run again, have sex without pain, or stop leaking every time she laughs.
Second, research your local market. Additionally, survey what other cash-based providers in your area are charging. Specifically, look at concierge medicine, cash-based PT, and pelvic health specialists. You will likely find a range of $150 to $250 per session for one-hour visits in most markets.
Third, price for the patient you want to attract. Moreover, a lower rate does not attract more committed patients — it attracts price-shoppers. The PelviBiz cash pay pricing guide covers this in full detail.
Phase 3 — Build your patient pipeline before you leave
This is the step most practitioners skip — and subsequently regret. You do not quit first and market second. You build your pipeline while you still have income security.
Specifically, here is what to build before your last insurance day:
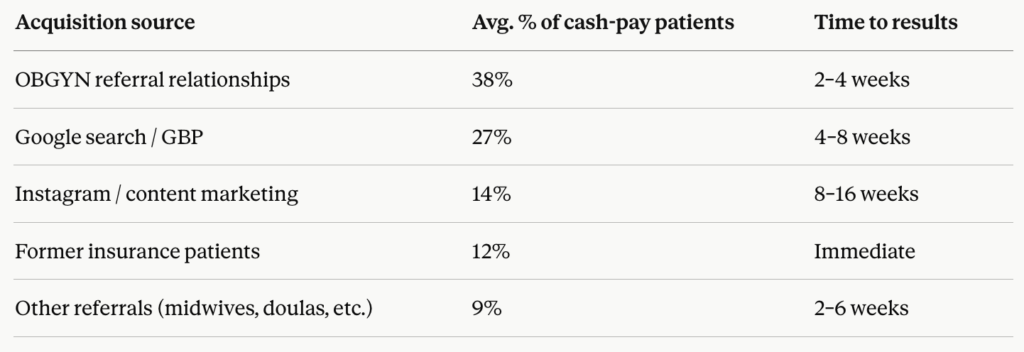
Your Google Business Profile. Fully optimized, with your specialty, your cash-pay model, and genuine patient reviews. This is your single highest-ROI marketing asset.
A referral relationship with at least one OBGYN. Pelvic health patients come from gynecology more than anywhere else. Furthermore, one strong OBGYN relationship can fill your schedule. The pelvic health OBGYN referral guide gives you the exact outreach framework.
A simple website with a clear call to action. You do not need a complicated funnel. However, you do need a page that explains who you help, what you do, and how to book.
An email list of interested patients. If you are transitioning from an existing practice, collect emails from patients who express interest in continuing with you in a cash-pay model. Many will follow you.
Phase 4 — Drop insurance panels strategically
You do not have to drop every panel at once. Consequently, many practitioners use a hybrid model for 6 to 12 months while building their cash-based caseload.
Here is the strategic sequence:
- First, drop the lowest-reimbursing plan. This frees up appointment slots and mental energy without dramatically affecting income.
- Second, add a cash-pay option for out-of-network patients. This tests your messaging and pricing with real patients.
- Third, track your cash-pay conversion rate. Specifically, if more than 60 percent of prospective patients who hear your cash-pay rate are booking, your pricing is either right or too low.
- Finally, drop additional panels as your cash caseload grows to replace the revenue.
This approach removes the all-or-nothing pressure that stops most practitioners from ever starting.
Phase 5 — Anchor your marketing to your clinical identity
Cash-based practices live and die on positioning. Therefore, you need to be known for something specific — not just “physical therapy” and not just “pelvic floor.”
Dr. Kelly Alhooie coined the term “OrthoPelvic” because she saw a gap: patients with pelvic floor dysfunction who also had orthopedic contributions to their symptoms. That specific positioning gave OrthoPelvic PT a reason to exist that no one else could claim.
Your positioning does not need to be as novel. However, it needs to be specific enough that the right patient — the one who will pay cash and commit to the process — immediately recognizes herself in your messaging.
The 90-Day Authority Plan inside PelviBiz is built specifically to help you develop and deploy that positioning in a structured timeframe.
What the transition actually looks like: a realistic timeline
Most practitioners who go through this process with a coach complete the full transition in 6 to 12 months. Here is a realistic timeline:
Months 1 to 2: Financial audit, pricing decision, first cash-pay patients booked. Months 3 to 4: First insurance panel dropped, referral relationships active, Google presence optimized. Months 5 to 6: Cash caseload at 50 percent or more. Second panel dropped. Months 7 to 12: Full cash-based model. Monthly revenue equal to or exceeding previous insurance income. Administrative hours cut by 60 to 80 percent.
This timeline assumes you have support. Specifically, practitioners who attempt this alone consistently take longer and make more expensive mistakes. The PelviBiz Growth Assessment is a free call that maps your specific situation to a realistic transition plan.
The mindset shift that makes or breaks the transition
Here is what nobody tells you: the hardest part of going insurance to cash pay is not the logistics. It is the identity shift.
Most clinicians were trained to believe that healthcare should be accessible to everyone, and that charging cash somehow conflicts with that value. However, the most accessible version of you is the one who is not burned out, not overbooked, and not cutting sessions short because the billing code runs out.
A study in JAMA found that physician burnout is directly correlated with administrative burden — the exact burden that insurance billing creates. Therefore, removing that burden is not a luxury. It is a clinical decision.
Furthermore, when you charge appropriately for your expertise, you stay in practice longer, you invest in continuing education, and you show up fully for every patient. That is accessibility at a different scale.
Common mistakes practitioners make during the transition
Underpricing from guilt. Setting a cash rate just above your insurance net rate is not a cash-pay practice — it is just a billing format change. Set your rate based on value and market positioning.
Dropping all panels at once. Unless you have a full cash caseload already, this creates a revenue cliff. Transition strategically.
Waiting to market until after the transition. Marketing takes time. Consequently, every week you delay building your pipeline is a week of revenue you will never recover.
Trying to do it alone. The practitioners who transition fastest are the ones with accountability, community, and a proven framework. That is exactly what the Power Circle Mastermind is built for.
Ready to make the transition?
The insurance to cash pay shift is not a gamble. It is a business decision — and like every business decision, it is most successful when it is planned, sequenced, and supported.
PelviBiz has coached 400-plus pelvic health practitioners through exactly this process. Moreover, every program — from the Power Circle Mastermind to 1:1 coaching — is built by someone who has done it, is still doing it, and knows the exact levers that move the needle in this specific niche.
Book Your Free Growth Assessment →
Q: How long does the insurance to cash pay transition typically take? Most practitioners complete the full transition in 6 to 12 months when following a structured framework. The timeline depends on your current caseload, your financial runway, and whether you are working with a coach. Practitioners who attempt the transition alone typically take longer and make more costly pricing and marketing mistakes.
Q: Do I have to drop all insurance panels at once to go cash pay? No. Most successful transitions use a phased approach — dropping the lowest-reimbursing panels first while building a cash-pay caseload in parallel. Going all-cash overnight without an existing patient pipeline creates unnecessary revenue risk.
Q: What cash pay rate should I charge as a pelvic health PT? Most cash-based pelvic health practitioners charge between $150 and $250 per one-hour session, depending on their market, specialization, and positioning. Your rate should be anchored to the value of your outcomes and your market context — not to what insurance reimburses. The PelviBiz cash pay pricing guide covers the full framework.
Q: Will I lose most of my patients when I go cash pay? You will lose some patients — typically those who were only seeing you because insurance covered it. However, the patients who remain tend to be more committed, more compliant, and more likely to refer others. Because your revenue per session increases significantly, you need far fewer patients to match or exceed your previous insurance income.




